When a hospital accreditation surveyor walks through your doors, one of the first things they assess is evidence that patients genuinely understand their care. Surveyors expect documented, measurable proof that patient education forms part of the clinical journey—not simply a printed leaflet left in a bedside drawer.
For hospitals pursuing CQC registration, JCI, CBAHI, or any other hospital accreditation programme, patient education is a core compliance requirement — not a secondary workstream.
In this guide explains what each major framework demands, how a compliant platform makes audit readiness a year-round standard, and what to prioritise when choosing a patient education solution for accredited hospitals.
What Each Accreditation Body Requires
Despite their differences in geography and scope, all major hospital accreditation frameworks share one principle: patient education must be a documented, standardised system.
In other words, education should never depend on the habits of individual clinicians or departments. Instead, hospitals must implement a structured process that ensures consistent delivery across the organisation.
| Body | Standard / Domain | Key Patient Education Requirement |
|---|---|---|
| CQC (England) | Caring & Responsive Domains | Person-centred, accessible information; documented consent & discharge education |
| JCI | PFE — Patient & Family Education | Assessed, culturally appropriate education with documented verification of understanding |
| CBAHI | Care of Patients (COP) | Formal education policy, multilingual materials, staff competency at every care transition |
| DNV GL | Patient Rights & Education | Individualised education plans, health literacy assessment |
| Accreditation Canada | Person-Centred Care | Education integrated into discharge planning and follow-up care |
CQC: Person-Centred Information and the Accessible Information Standard
For NHS trusts and independent providers registered with the CQC, the Caring and Responsive domains of the Five Key Questions framework require that patients receive information they can understand — in their language, at an appropriate literacy level, and in an accessible format.
Under the CQC’s Single Assessment Framework, introduced in 2024, inspectors assess patient education through Quality Statements that place greater emphasis on personalised, outcome-focused care rather than process compliance alone.
Additionally, the Accessible Information Standard (AIS) places additional statutory obligations on providers to identify and meet individual communication needs. Materials accredited by PIF TICK — the UK’s patient information quality mark, held by AMPM Training’s MINT PILs — provide directly relevant and independently validated evidence for CQC inspections and AIS compliance.
JCI: Verified Understanding, Not Just Delivery
JCI’s Patient and Family Education (PFE) standards require that hospitals assess each patient’s literacy level, language preference, and cultural background before education is delivered.
However, JCI goes further than many frameworks. Hospitals must also document proof that patients understood the information provided. In practice, clinicians typically verify understanding through teach-back or similar methods.
This requirement applies uniformly across every department and care setting. Inconsistency between departments is among the most frequently cited PFE findings during JCI surveys, particularly in hospitals where education relies on individual clinician initiative rather than a standardised, system-level workflow.
By contrast, hospitals that use an EMR-integrated education platform standardise delivery across departments and eliminate these variations.
CBAHI: Multilingual Readiness as a Compliance Requirement
For hospitals in Saudi Arabia, CBAHI’s Care of Patients domain requires a formal written education policy, documentation at every care transition — admission, procedure, discharge, and follow-up.
In addition, hospitals must provide multilingual materials for diverse patient populations. Many Gulf hospitals therefore need education resources in Arabic, Urdu, Tagalog, Hindi, and other commonly used languages.
A patient education standardisation framework that cannot accommodate this linguistic diversity will fail CBAHI review regardless of the quality of the underlying clinical care.
Multilingual content must be clinically validated, not machine-translated, and must be demonstrably appropriate for the health literacy levels of the populations served.
DNV GL and Accreditation Canada: Education Embedded in Individual Care Plans
DNV GL’s hospital standards require individualised education plans informed by health literacy assessments, treating patient education as a component of personalised care rather than a one-size-fits-all discharge checklist. Accreditation Canada’s Qmentum framework similarly positions education as integral to person-centred care, with specific expectations around discharge planning and post-discharge follow-up. For hospitals operating across multiple countries or seeking dual accreditation, a single platform capable of meeting both frameworks simultaneously significantly reduces administrative complexity.
How a Structured Platform Makes Compliance the Default
Hospitals that approach hospital accreditation as a documentation exercise — gathering evidence in the weeks before a survey — are exposed. Surveyors are trained to identify whether patient education is genuinely embedded in clinical workflow or prepared for the visit. A structured, technology-enabled platform addresses this at its root by making compliance continuous.
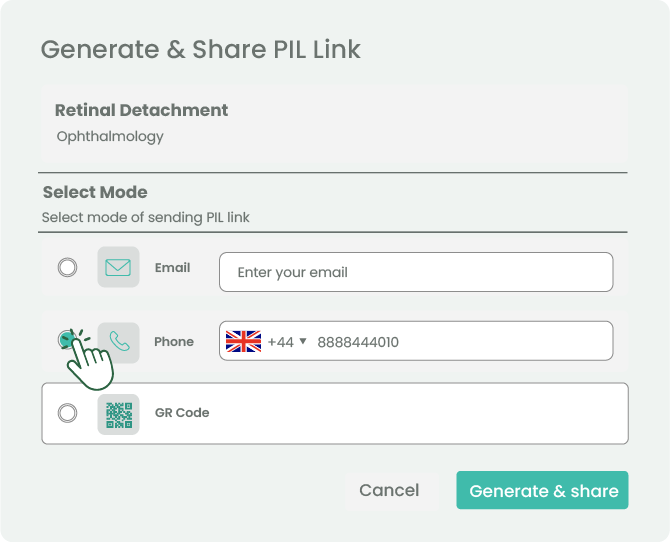
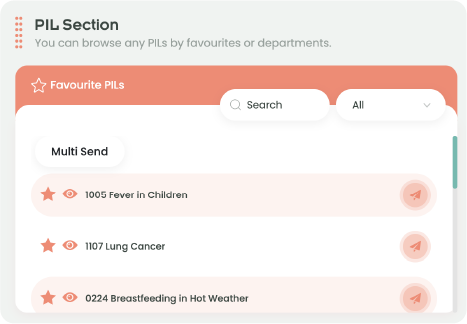
- Consistent delivery across departments: A shared, validated content library eliminates the variation between wards and specialties that inspectors most commonly flag. Every clinician works from the same accreditation-ready materials, removing the risk that one department’s practices undermine an otherwise strong survey result.
- Automatic documentation in the patient record: EMR-integrated delivery logs every interaction — what was sent, to which patient, by which clinician, and when — creating an auditable trail without adding administrative burden to clinical staff. This single feature resolves the most common documentation gap found during patient education audits.
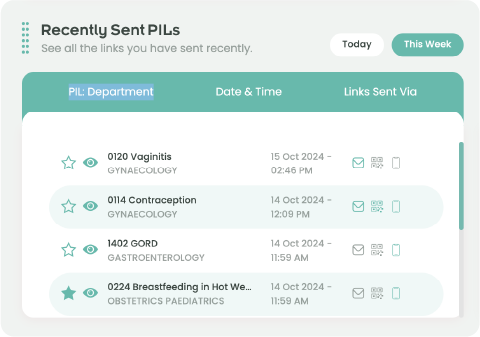
- Measurable engagement data: An analytics dashboard showing delivery rates, topic-level access, and department-by-department performance provides the institutional evidence that modern hospital accreditation standards increasingly require. Surveyors expect to see not just that education occurred, but that it reached patients and was tracked.
- Scalable across sites: For hospital networks and multi-site groups, a centralised platform ensures that accreditation readiness is consistent across every location — not dependent on the practices of individual site managers or clinical leads.
| ROI BEYOND THE SURVEY ✓ 15–30% reduction in unplanned readmissions with structured patient education (published evidence range) ✓ Fewer formal complaints: the majority relate to communication failures that standardised education addresses directly ✓ Staff time reclaimed from manual, inconsistent education delivery ✓ Stronger survey outcomes: compliant hospitals report more confident, faster accreditation cycles |
Five Criteria for Choosing a Compliant Patient Education Platform
- Independently accredited content: Is the material quality-marked by a recognised body? MINT PILs hold PIF TICK accreditation and are reviewed by NHS consultants across 24+ specialties in Arabic and English. Independent accreditation removes the burden on your clinical governance team to validate every piece of content internally.
- Multilingual capability: Can materials be delivered in the languages your patient population requires without relying on third-party translation tools? For CBAHI and JCI hospital accreditation, multilingual delivery must be built into the platform workflow, not handled as a manual workaround.
- EMR integration with ICD-10 triggering: Does the platform automate delivery at defined clinical milestones, removing the dependency on individual staff action? Trigger-based delivery ensures no patient is missed regardless of ward or shift.
- Analytics and reporting: Can the platform generate delivery rates, engagement data, and department-level reports at the click of a button? The ability to produce an accreditation evidence pack on demand is an increasingly common surveyor expectation.
- Implementation speed: Can the system go live across departments without a lengthy IT project? For hospitals approaching a survey cycle, time-to-deployment is often as important as feature depth.
MINT Executive — AMPM Training’s enterprise-tier platform — meets each of these criteria for large hospitals and multi-site networks.
Accreditation Is a Standard, Not an Event
Hospitals that sustain hospital accreditation — whether CQC, JCI, or CBAHI — do not treat it as an annual event. They embed its standards into daily clinical operations, making compliance the path of least resistance rather than a pre-survey effort.
When patient education becomes part of the clinical workflow, compliance naturally follows. Conversely, organisations that attempt to reconstruct documentation shortly before a survey often struggle.
A structured patient education system built for hospital accreditation is not a compliance cost. It is a clinical and operational asset that improves outcomes, reduces institutional risk, supports staff in delivering consistent care, and provides the documentation foundation every survey demands — year-round, not just at inspection time.
| Ready to Build an Accreditation-Ready Patient Education System? MINT Platform by AMPM Training is trusted by hospitals seeking CQC, JCI, CBAHI, and global accreditation. Deploy in days, not months, with direct EMR integration and a full analytics dashboard. Request a demo |
References
The following sources underpin the accreditation requirements, clinical evidence, and quality standards cited in this article.
Accreditation Standards
[1] Joint Commission International (JCI). Accreditation Standards for Hospitals and Academic Medical Centers, 8th Edition. Effective 1 January 2025.
[2] Central Board for Accreditation of Healthcare Institutions (CBAHI). National Hospital Standards, 3rd Edition (effective 1 January 2016)
[3] Care Quality Commission (CQC). Single Assessment Framework and Five Key Questions. Updated 2024.
[4] NHS England. Accessible Information Standard (AIS), 2016 (under review).
[5] Patient Information Forum (PIF). PIF TICK — UK Quality Mark for Health Information (120+ accredited creators as of March 2024).
Clinical Evidence — Readmission Reduction
[6] Cañon-Montañez W, Duque-Cartagena T, Rodríguez-Acelas AL. Effect of Educational Interventions to Reduce Readmissions due to Heart Failure Decompensation in Adults: a Systematic Review and Meta-analysis. Invest Educ Enferm. 2021;39(2):e05. PMID: 34214282.
[7] Becker C, et al. Interventions to Improve Communication at Hospital Discharge and Rates of Readmission: A Systematic Review and Meta-analysis. JAMA Network Open. 2021;4(8):e2119346. PMID: 34448868.
[8] Oh EG, et al. Effectiveness of Discharge Education with the Teach-Back Method on Readmission among Heart Failure Patients: A Systematic Review and Meta-analysis. Patient Educ Couns. 2022 Nov. PMID: 36244866.